Edit (2): I ran logistic regression models in R to see how well each predicted the output. tl/dr: there's nothing between them.
Here's my code:
d <- read.csv("Copy of Cancer data - Weightings.csv")
mrc <- glm(cancer ~ weightrc, data = d, family = "binomial")
mun <- glm(cancer ~ unweight, data = d, family = "binomial")
mca <- glm(cancer ~ weightca, data = d, family = "binomial")
mic <- glm(cancer ~ weightic, data = d, family = "binomial")
d$prc <- predict(mrc, type = "response")
d$pun <- predict(mun, type = "response")
d$pca <- predict(mca, type = "response")
d$pic <- predict(mic, type = "response")
par(mfrow = c(2, 2))
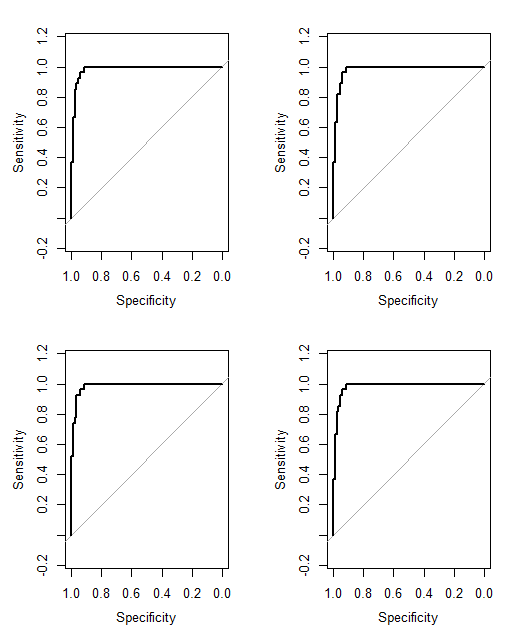
roc(d$cancer, d$prc, ci = TRUE, plot = TRUE)
roc(d$cancer, d$pun, ci = TRUE, plot = TRUE)
roc(d$cancer, d$pca, ci = TRUE, plot = TRUE)
roc(d$cancer, d$pic, ci = TRUE, plot = TRUE)
And the output:
> par(mfrow = c(2, 2))
> roc(d$cancer, d$prc, ci = TRUE, plot = TRUE)
Call:
roc.default(response = d$cancer, predictor = d$prc, ci = TRUE, plot = TRUE)
Data: d$prc in 81 controls (d$cancer 0) < 27 cases (d$cancer 1).
Area under the curve: 0.9831
95% CI: 0.9637-1 (DeLong)
> roc(d$cancer, d$pun, ci = TRUE, plot = TRUE)
Call:
roc.default(response = d$cancer, predictor = d$pun, ci = TRUE, plot = TRUE)
Data: d$pun in 81 controls (d$cancer 0) < 27 cases (d$cancer 1).
Area under the curve: 0.9808
95% CI: 0.9602-1 (DeLong)
> roc(d$cancer, d$pca, ci = TRUE, plot = TRUE)
Call:
roc.default(response = d$cancer, predictor = d$pca, ci = TRUE, plot = TRUE)
Data: d$pca in 81 controls (d$cancer 0) < 27 cases (d$cancer 1).
Area under the curve: 0.9854
95% CI: 0.9688-1 (DeLong)
> roc(d$cancer, d$pic, ci = TRUE, plot = TRUE)
Call:
roc.default(response = d$cancer, predictor = d$pic, ci = TRUE, plot = TRUE)
Data: d$pic in 81 controls (d$cancer 0) < 27 cases (d$cancer 1).
Area under the curve: 0.9822
95% CI: 0.9623-1 (DeLong)