I'm dealing with survival data which comes from hospital records. All the patients were diagnosed with cancer. During their stay at the hospital, patients are enrolled in treatment protocols (to receive chemotherapy drugs/regimens). A patient may stop his protocol early for several reasons: progression (the size of the tumors increased or a new tumor appeared), complications or death. It is quite common that patients withdraw from their treatment protocols because clinicians observed a significant progression of their cancer and start a different treatment protocol days/weeks after. The figure below illustrates the survival data for a few patients. 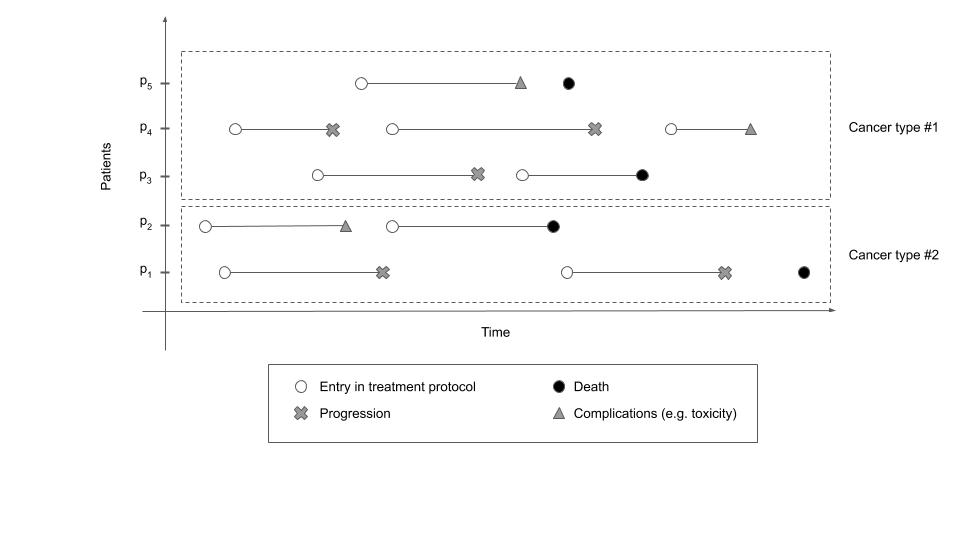
Using this data, I want to predict Progression-Free Survival (PFS), which is defined as the time from study entry (the date of the 1st treatment protocol) to the event of interest: progression or death.
How shall I deal with such data?
Since I'm quite new to survival analysis, I was going to use the coxph function in R but first, I want to be sure I understand what's going on and have the right method.
Here are my thoughts so far:
The entry time is different for each individual (the data does not come from a RCT - Randomized Clinical Trial - and, as a result, there is no obvious reference time). This is a case of delayed entry (left truncation). This answer explains what is the right syntax for the
coxphfunction (and how the dataset should be converted to a count process first by using thesurvSplitfunction from thesurvivalpackage).About censoring: some individuals (such as individual p4) have not progressed or died during the observation period. This is a case of right censoring. Intuitively, I would have said that we only have right censoring. However, this paper which deals with prediction of PFS in a similar setting suggests that, when individuals have progressed (or died), the data is interval-censored (the event of interest is assumed to occur between the last visit without progression and the first visit showing disease progression). Shall I follow the suggestion of the authors and use methods for interval-censored data?
Many individuals (such as individuals p1 or p4) have multiple events of "progression". How shall I account for these multiple events? Following this answer, I would have a
cluster(orfrailty) term to account for repeated events per individuals and I could also have astrata(cancer_type)term to allow for different baseline functions per cancer types (there are two different cancer types in the figure above). In this article, the authors suggest different methods to deal with recurrent events (extensions of the classical cox PH model such as the "Andersen Gill model" or the "Prentice, William and Petersen model"). Is this the right way to go?