You are not gonna get an answer
Exactly predicting the influence of effects such as mutated strains is extremely difficult. Even governments with lot's of mathematicians and big computers working for them are not well capable of making good predictions (or even bad predictions).
Predicting the course of Covid is like predicting the weather more than 14 days ahead of time but with very inaccurate models and inaccurate measurements.
You are gonna get an answer
Intuition of the mechanics by means of a game
If your goal with this question is just to gain some insight into the underlying theoretical considerations then you might get some improvements in your intuition.
In this part of the question, I am gonna give some intuition by replacing viruses with dice. I am actually currently making a board game that includes the aspect of virus mutations, and now even my 5-year-old son "understands" the aspects of the mechanics and aspects of probability for an epidemic.

The game mimics transmission by rolling several dice. When you roll a six then an infection occurs. When you roll 2/3 or more sixes then the newly infected person gets a headache as well (2 when it's an adult, 3 for kids).
Let's see what the probability is for rolling at least 1 six.
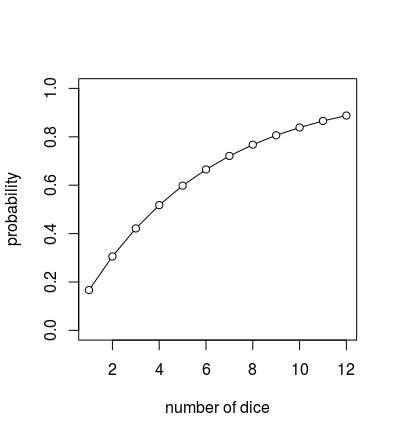
Note: It is not linear! Reducing transmissibility rate by $x \%$ (changing the number of dice, the viral load) may not be the same reduction in transmissibility probability per contact.
In this game, the virus variant will increase the number of dice used in the infection by 'two dice' (in a real-world the variant might also increase the rate of infection, the viral load, in some way).
Already for this very basic game, it is very difficult to compute the effect of the variant (the two extra dice). There are several ways in which the effect of higher infectivity will have different effects that vary due to inhomogeneities.
When you change the number of dice from 10 to 12 then the effect (probability increases a bit from 84% to 89%) is a lot different from when you change the number of dice of 1 to 3 (Increase from 17% to 42%, more than doubled).
There are several ways in which increased infectivity will have inhomogeneous effects. The effect of increased infectivity is for this game the largest when the infectivity is low (I believe the same will be true for the real world). When the probability of infection is high, for instance inside families, then people are gonna get sick anyway (at least with high probability).
(The same is true for the interventions/measures like mask-wearing that are in the opposite direction as the virus variant; For these as well the effects will be variable and depend on the situation. There is another question here where this came across as well.)
The types of spread and the population are inhomogeneous. Some areas are more crowded than others, have more complex networks with bigger knots, etc. Because of these, you may have different effects of the increased transmissibility of the variant (the increase of dices).
It is wrong to think of some virus mutation to increase the R(t) value (the reproduction number) or the transmissibility rate or transmissibility probability.
Those figures eventually are just based on an estimated/observed growth rate that is rescaled to express the reproduction scale.
The growth rate might is not the same as transmissibility, and transmissibility is not the same as what changed in the virus mutant. The underlying mechanisms are complex, inhomogeneous, and change from place to place. The growth rate, or other related statistics, is just what is observed at the surface, but it is something inside the machinery that has changed.
In short
The effect of a virus mutant is not easily determined.
Let alone that the effect can be predicted/extrapolated. But what people (politicians and media) do is just extrapolate the observed effects of the mutant to other populations (without considering the mechanics and the idea that the effects may be different for different situations).
For example, in South East England scientists observe some increase of a variant. Subsequently, it became the dominant strain in London.
Then people start to use the same figures (like R value increases such and such) and plug it into their own simple model as if this effect on the surface (a particular increase of the R value) is gonna be exactly the same.
I believe that this is not the right way to handle the lack of information. The correct way is to gather more/richer/better data (and that is what people did afterward, and they found in many other places that the variant is not as strongly fast-spreading, or sometimes they found no effect at all.).
a vaccine that is 80% efficacious against a new strain, but that new strain is 80% more transmissible
...
what is the estimated net outcome in case rates
...
Is it zero?
Typically the vaccine/immunity is gonna have more effect.
In the basic SIR model, the effective reproduction number is often compared with the basic reproduction number along with the fraction of people that are not immune (non-susceptible) (the ratio of the total susceptible people $S$ over the total number of people $N$)
$$R(t) = R_0 \cdot S/N$$
So vaccination is gonna reduce that number $S$ and mutations are gonna increase $R_0$. However, the number $R_0$ does not increase linearly with an increase of transmissibility, it will be less.