everyone!
I want to do overall Recurrence-free survial analysis for one continuous predictor with Kaplan-Meier method, but the determination of the cut-point for groups really confused me.
Most related references I've read tended to adopt the median of the predictor as the group's cut point. However, some posts in this forum recommended the cutp()function in SurvMisc package to choose the optimal cut-point.
I tried both, but the results had a big difference. The plots below show the variance.
The first plot used `cutp()`function to choose the optimal cut-point; the second plot used median method to select the cut-point.
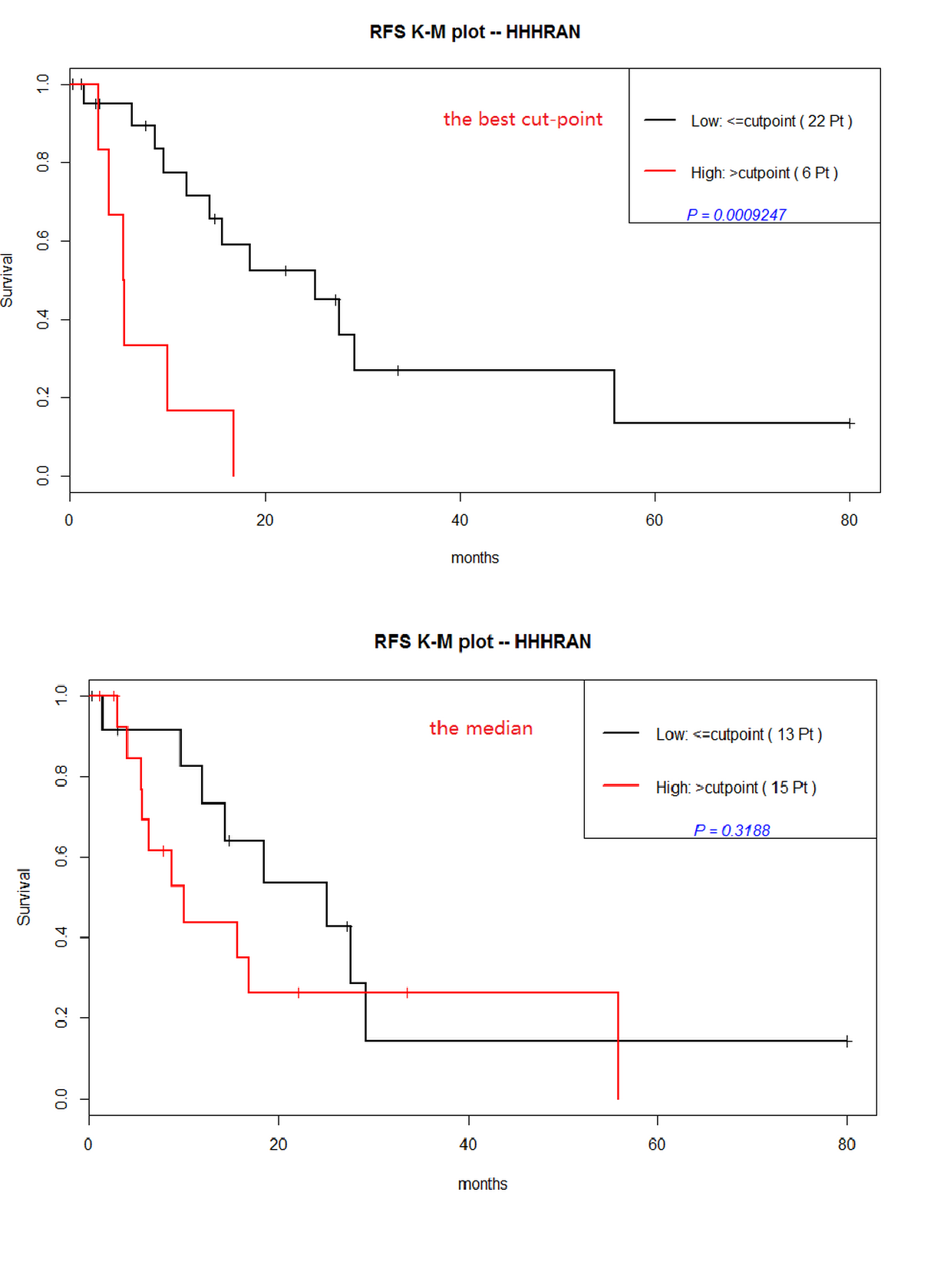
The first KM plot with the optimal cut-point demonstrated that the continuous predictor "HHHRAN" was statistically significant ($p=0.0009247$); however, the second plot with median cut-point showed the predictor was not significant($p=0.3188$).
Besides, We observed a clear contrast between the number of patients in resultant groups with two methods: the Optimal cut-point (low,22 patients;high,6 patients) and the median cut-point (low,13 patients;high,15 patients). There was a obvious bias in the first groups (22 vs 6).
So, my questions were:
- Is the result in first method(the optimal cut-point) reliable? (Due to the bias in groups.... ). If the larger samples performed, how did it come out? More reliable compare to the small samples? But still a big bias in numbers(207 vs 104)...
larger samples in optimal cut-point method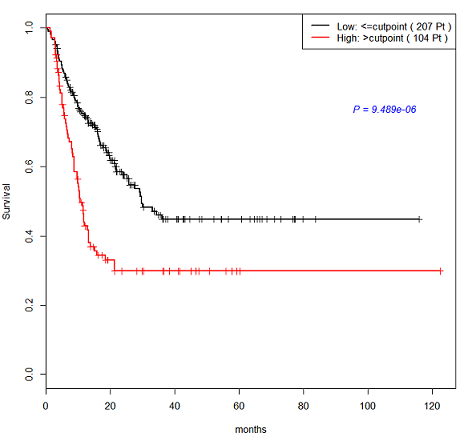
- Can anyone list some research papers which used the optimal cut-point in survival analysis? I have tried in google,but few.
Any suggestion would be a great appreciate! Thanks in advance!